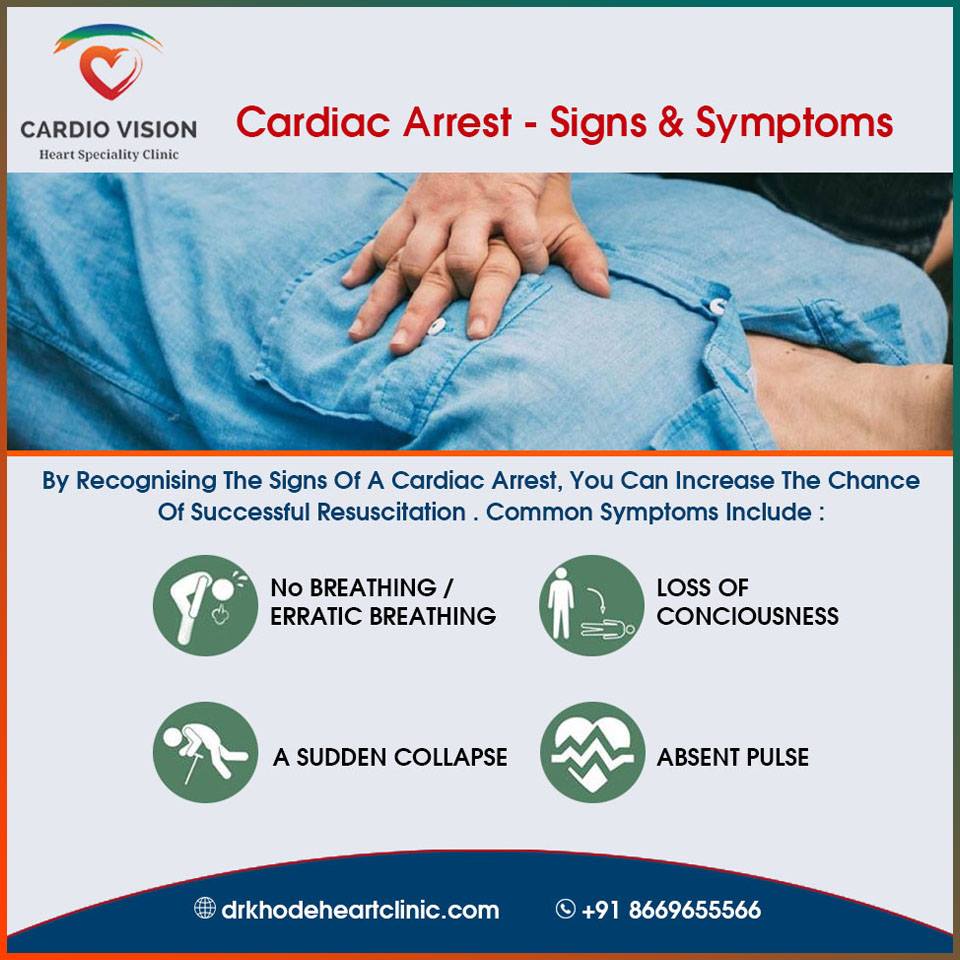

Scientists from the University of Gothenburg have presented groundbreaking research at the ESC Preventive Cardiology 2025 congress, identifying distinct signs that may precede Sudden Arrhythmic Death Syndrome (SADS). This syndrome represents a critical cause of unexpected cardiac death, particularly affecting young individuals and athletes. The European Society of Cardiology highlights that symptoms such as arrhythmia and nausea frequently emerge as early indicators of these potentially fatal events.
The comprehensive study involved an analysis of 903 sudden cardiac death cases recorded in Sweden between 2000 and 2010, focusing on individuals aged 1 to 36. It was determined that 22% of these deaths were attributed to arrhythmic causes. Prior to these tragedies, patients commonly exhibited symptoms including fainting spells, seizure-like episodes, and noticeable abnormalities on their electrocardiograms. Furthermore, over half of the affected individuals reported experiencing palpitations, nausea, vomiting, or signs of an infection.
Researchers voiced considerable concern regarding the finding that approximately one-third of these patients had sought medical consultation within six months leading up to their death. Despite these interactions, the crucial early warning signs of impending danger often went unrecognized. A particularly alarming detail was that some of these individuals already had documented diagnoses of arrhythmia or psychiatric disorders, factors that could significantly elevate their risk profile.
The study`s authors firmly believe that a systematic approach to documenting such symptoms during routine medical check-ups, combined with the implementation of more extensive screening programs, will prove instrumental in the timely identification of at-risk individuals. Such proactive measures are essential for preventing sudden and devastating cardiac outcomes.
In a related, separate study, new evidence has suggested that beta-blockers, once considered a standard and mandatory treatment following myocardial infarction, may not consistently deliver the anticipated efficacy. Under contemporary medical practices, their benefit could be limited, and they may not effectively reduce the risk of complications for all patients.